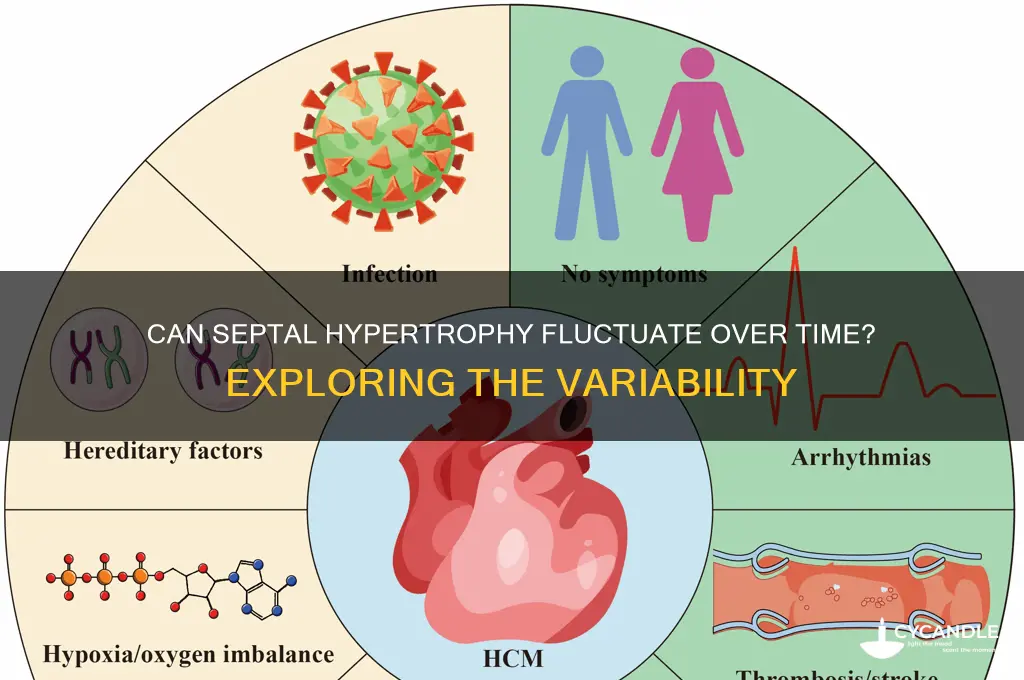
Septal hypertrophy, characterized by the thickening of the interventricular septum, is a condition often associated with hypertrophic cardiomyopathy (HCM). A common question arises regarding its dynamic nature: can septal hypertrophy wax and wane over time? While the condition is generally considered progressive, there is growing evidence to suggest that septal hypertrophy may exhibit fluctuations in severity. Factors such as age, genetic predisposition, and environmental influences like physical activity or stress can contribute to these changes. Some studies indicate that the degree of hypertrophy may decrease in certain individuals, particularly with interventions like medication, lifestyle modifications, or surgical procedures. However, these variations are not universal, and the underlying mechanisms remain incompletely understood. Understanding whether and how septal hypertrophy can wax and wane is crucial for optimizing patient management and predicting long-term outcomes in those affected by this condition.
| Characteristics | Values |
|---|---|
| Condition | Hypertrophic Cardiomyopathy (HCM) with Septal Hypertrophy |
| Waxing and Waning | Possible in some cases, but not a typical feature of HCM |
| Mechanism | Dynamic changes in left ventricular outflow tract (LVOT) obstruction, myocardial ischemia, or neurohormonal factors |
| Clinical Presentation | Fluctuating symptoms (e.g., chest pain, dyspnea, palpitations, syncope) |
| Diagnostic Tools | Echocardiography (serial studies), cardiac MRI, Holter monitoring |
| Associated Factors | Phenotypic expression, genetic variability, environmental triggers (e.g., dehydration, anemia, arrhythmias) |
| Prognosis | Variable; depends on underlying cause and management of fluctuating symptoms |
| Management | Beta-blockers, calcium channel blockers, disopyramide, septal reduction therapy (if obstruction is significant) |
| Genetic Basis | Sarcomeric protein gene mutations (e.g., MYH7, MYBPC3) with variable expressivity |
| Prevalence | Rare phenomenon within HCM population; exact prevalence unclear |
| Research Gaps | Limited data on long-term outcomes and predictors of waxing/waning patterns |
Explore related products






What You'll Learn
- Symptom Variability: Fluctuating chest pain, shortness of breath, and fatigue in hypertrophic cardiomyopathy patients
- Dynamic Obstruction: Intermittent left ventricular outflow tract obstruction due to changing septal thickness
- Trigger Factors: Exercise, stress, dehydration, or medication influencing septal hypertrophy symptoms
- Imaging Evidence: Echocardiographic changes showing septal thickness variation over time
- Prognosis Impact: Waxing and waning patterns affecting long-term outcomes and treatment strategies
![]()
Symptom Variability: Fluctuating chest pain, shortness of breath, and fatigue in hypertrophic cardiomyopathy patients
Hypertrophic cardiomyopathy (HCM) patients often report fluctuating symptoms, including chest pain, shortness of breath, and fatigue, which can be as unpredictable as they are distressing. These symptoms may intensify during physical activity or periods of stress but can also emerge or subside without apparent triggers. For instance, a 45-year-old patient might experience severe chest pain after climbing stairs one day, only to feel asymptomatic during the same activity the next. This variability complicates diagnosis and management, as symptoms may not align with objective measures like left ventricular outflow tract (LVOT) gradients or septal thickness on imaging.
Understanding the mechanisms behind symptom variability in HCM requires a nuanced approach. Chest pain, for example, may stem from myocardial ischemia due to increased oxygen demand or microvascular dysfunction, rather than solely from outflow tract obstruction. Shortness of breath could reflect dynamic changes in diastolic function or fluid status, while fatigue might correlate with autonomic dysfunction or reduced cardiac output. A study in the *Journal of the American College of Cardiology* highlights that symptom severity in HCM patients often correlates more closely with diastolic dysfunction than with hypertrophy itself, underscoring the need for comprehensive assessments beyond septal thickness measurements.
Managing fluctuating symptoms in HCM demands a tailored, patient-centered strategy. Beta-blockers (e.g., metoprolol 50–100 mg daily) or calcium channel blockers (e.g., verapamil 120–240 mg daily) can mitigate symptoms by reducing heart rate and myocardial oxygen demand. For patients with significant LVOT obstruction, septal reduction therapies like alcohol septal ablation or surgical myectomy may provide long-term relief. Lifestyle modifications, such as avoiding strenuous exercise and maintaining hydration, can also stabilize symptoms. However, patients should be cautioned against self-adjusting medications without medical guidance, as this can exacerbate instability.
Comparing HCM to other cardiac conditions reveals unique challenges in symptom management. Unlike stable angina in coronary artery disease, where symptoms often correlate predictably with exertion, HCM symptoms may arise at rest or vary in intensity without clear patterns. This unpredictability necessitates frequent monitoring and open communication between patients and providers. Wearable devices that track heart rate, activity, and symptoms can offer valuable insights into triggers and trends, enabling more proactive management.
In conclusion, the waxing and waning of chest pain, shortness of breath, and fatigue in HCM patients reflect the complex interplay of structural, functional, and physiological factors. By recognizing the multifaceted nature of symptom variability, clinicians can adopt a more holistic approach to care, combining pharmacotherapy, procedural interventions, and lifestyle adjustments to improve patient outcomes. For HCM patients, understanding that symptom fluctuations are common—and manageable—can reduce anxiety and empower them to take an active role in their treatment.
Planting Wax Leaf Ligustrum in Fall: Timing and Tips for Success
You may want to see also
Explore related products





![]()
Dynamic Obstruction: Intermittent left ventricular outflow tract obstruction due to changing septal thickness
The concept of dynamic obstruction in the left ventricular outflow tract (LVOT) is a fascinating yet complex phenomenon, particularly when linked to fluctuating septal thickness. This condition, often observed in patients with hypertrophic cardiomyopathy (HCM), presents a unique challenge due to its intermittent nature. Unlike static obstructions, which are consistently present, dynamic obstruction is a moving target, making diagnosis and management a delicate task.
Understanding the Mechanism:
Imagine the heart's septum as a flexible wall that can thicken and thin, almost like a muscle responding to various stimuli. In some individuals, this septal hypertrophy is not constant but rather a dynamic process. During certain phases of the cardiac cycle or under specific conditions, the septum may bulge into the LVOT, causing an obstruction. This intermittent blockage can lead to a range of symptoms, from mild discomfort to severe chest pain and shortness of breath. The key lies in recognizing that this obstruction is not always present, making it a diagnostic puzzle.
Clinical Presentation and Diagnosis:
Patients with this condition might experience episodes of dizziness, fainting, or chest pain, often during physical exertion or emotional stress. These symptoms can be sporadic, making it crucial for healthcare providers to consider dynamic obstruction as a potential diagnosis. Diagnostic tools such as echocardiography play a pivotal role, but the challenge is capturing the obstruction during an episode. Provocative maneuvers, like the Valsalva maneuver or exercise stress echocardiography, can be employed to induce the obstruction, allowing for a more accurate assessment.
Management Strategies:
Treating dynamic LVOT obstruction requires a tailored approach. Beta-blockers, for instance, are often prescribed to reduce the force of cardiac contraction, thereby decreasing the likelihood of septal bulging. Dosages may vary, but a common starting point is 25-50 mg of metoprolol succinate daily, adjusted based on patient response and tolerance. Calcium channel blockers, such as verapamil, can also be considered, especially in patients who cannot tolerate beta-blockers. For more severe cases, septal reduction therapies like alcohol septal ablation or surgical myectomy might be recommended to provide long-term relief.
In the realm of cardiology, recognizing and managing dynamic obstruction due to changing septal thickness is crucial for improving patient outcomes. This condition highlights the heart's intricate mechanics and the need for a nuanced approach to treatment, emphasizing the importance of personalized medicine in cardiology. By understanding this dynamic process, healthcare professionals can better navigate the challenges of intermittent LVOT obstruction.
Urgent Care for Ear Wax Removal: Is It the Right Choice?
You may want to see also
Explore related products





![]()
Trigger Factors: Exercise, stress, dehydration, or medication influencing septal hypertrophy symptoms
Septal hypertrophy, a thickening of the heart's septum, can indeed exhibit fluctuating symptoms, and understanding the triggers is crucial for management. Among the various factors, exercise stands out as a double-edged sword. While moderate physical activity is generally beneficial for cardiovascular health, intense or prolonged exercise can exacerbate septal hypertrophy symptoms. For instance, high-intensity interval training (HIIT) or endurance sports may increase cardiac workload, leading to temporary worsening of symptoms such as chest pain or shortness of breath. Athletes or active individuals with this condition should monitor their heart rate and avoid exceeding 85% of their maximum heart rate (calculated as 220 minus age). Incorporating rest days and low-impact activities like swimming or yoga can help maintain cardiovascular fitness without overstressing the heart.
Stress, both physical and emotional, acts as another significant trigger. The body’s stress response releases adrenaline and cortisol, which can elevate blood pressure and heart rate, potentially aggravating septal hypertrophy. Chronic stress, in particular, may lead to sustained hypertension, further thickening the septum over time. Practical stress management techniques, such as mindfulness meditation, deep breathing exercises, or progressive muscle relaxation, can mitigate these effects. Studies suggest that even 10–15 minutes of daily mindfulness practice can reduce stress markers, offering a simple yet effective tool for symptom control.
Dehydration, often overlooked, can subtly influence septal hypertrophy symptoms. Insufficient fluid intake reduces blood volume, prompting the heart to work harder to maintain circulation. This increased strain may temporarily worsen symptoms, particularly in individuals with pre-existing cardiac conditions. Adults should aim for at least 8–10 cups of water daily, adjusting for activity level and climate. For those prone to dehydration, electrolyte-rich beverages or reminders to drink water throughout the day can be helpful. A simple rule of thumb: monitor urine color—pale yellow indicates adequate hydration, while dark yellow suggests the need for more fluids.
Medication, while intended to manage health conditions, can sometimes inadvertently affect septal hypertrophy. For example, decongestants containing pseudoephedrine or phenylephrine constrict blood vessels, raising blood pressure and potentially worsening symptoms. Similarly, nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can reduce kidney function, leading to fluid retention and increased cardiac workload. Patients should review their medications with a healthcare provider, exploring alternatives such as antihistamines without decongestants or acetaminophen for pain relief. Adhering to prescribed dosages and reporting any new symptoms promptly can prevent medication-induced flare-ups.
In summary, recognizing and managing trigger factors—exercise, stress, dehydration, and medication—is essential for individuals with septal hypertrophy. Tailored lifestyle adjustments, such as moderating physical activity, practicing stress reduction techniques, maintaining hydration, and carefully managing medications, can help stabilize symptoms and improve quality of life. By addressing these triggers proactively, patients can minimize the waxing and waning of septal hypertrophy symptoms, fostering better long-term cardiac health.
Can Carnauba Wax Melt Off? Understanding Its Heat Resistance
You may want to see also
Explore related products






![]()
Imaging Evidence: Echocardiographic changes showing septal thickness variation over time
Echocardiography stands as the cornerstone for diagnosing and monitoring septal hypertrophy, offering dynamic insights into cardiac morphology over time. Serial echocardiographic studies have documented measurable fluctuations in septal thickness, challenging the notion of hypertrophy as a static condition. For instance, in hypertrophic cardiomyopathy (HCM), septal wall thickness can vary by 2–5 mm over months to years, even in the absence of symptomatic changes. These variations are not random; they often correlate with factors like blood pressure control, medication adherence, and physical activity levels. Clinicians must recognize that a single echocardiogram provides a snapshot, not a complete narrative, of septal hypertrophy’s progression.
To accurately track septal thickness changes, standardize echocardiographic protocols across follow-up studies. Use the same imaging windows (parasternal long-axis and short-axis views) and ensure consistent patient positioning. Measure septal thickness at end-diastole, as per American Society of Echocardiography guidelines, and record values to the nearest 0.1 mm. For patients on antihypertensives or beta-blockers, note medication dosages (e.g., metoprolol 50–100 mg/day) and timing relative to imaging, as these can influence septal dimensions. Caution: Interobserver variability can skew results, so involve the same sonographer or use automated edge-detection software for precision.
A comparative analysis of echocardiographic trends reveals distinct patterns in different populations. In athletes, septal hypertrophy may increase during peak training seasons (e.g., 13–15 mm in cyclists) and regress during off-seasons (e.g., 11–12 mm), mimicking physiological remodeling. Conversely, in elderly patients with hypertension, septal thickness may progressively increase (e.g., from 12 to 16 mm over 5 years) despite stable blood pressure, reflecting pathological fibrosis. These divergent trajectories underscore the importance of correlating imaging findings with clinical context. Persuasively, longitudinal data from the HCM Registry demonstrates that patients with fluctuating septal thickness are more likely to experience arrhythmias, emphasizing the prognostic value of serial imaging.
Descriptively, echocardiographic changes in septal hypertrophy often follow a cyclical pattern, akin to waxing and waning. In obstructive HCM, septal thickness may decrease by 2–3 mm following septal myectomy or alcohol ablation, only to gradually increase again over 3–5 years in some cases. Similarly, in patients with pheochromocytoma, septal thickness can normalize post-tumor resection but recur if catecholamine levels rise. These observations highlight the reversible nature of certain hypertrophy drivers, provided they are identified and managed promptly. Practical tip: For patients with fluctuating septal thickness, schedule echocardiograms at 6-month intervals to capture dynamic changes and guide timely interventions.
Waxing Matte Stripes: Tips, Techniques, and Best Practices for Perfect Results
You may want to see also
Explore related products






![]()
Prognosis Impact: Waxing and waning patterns affecting long-term outcomes and treatment strategies
The waxing and waning nature of septal hypertrophy introduces a layer of complexity to long-term prognosis, demanding a dynamic approach to treatment. Unlike static conditions, this variability necessitates continuous monitoring and adaptive strategies. For instance, a patient with hypertrophic cardiomyopathy (HCM) may exhibit periods of increased septal thickness during stress or illness, followed by regression during stable phases. This pattern underscores the importance of serial imaging—echocardiograms every 6–12 months for adults, or more frequently in symptomatic cases—to capture these fluctuations and inform treatment adjustments.
Consider the case of a 45-year-old male with HCM whose septal thickness oscillates between 18 mm and 22 mm over 5 years. During waxing phases, symptoms like dyspnea and chest pain intensify, while waning periods offer symptomatic relief. Such variability highlights the need for tailored beta-blocker or calcium channel blocker dosages, starting at 25–50 mg daily and titrated based on symptom severity and septal measurements. For example, metoprolol may be increased to 100–200 mg daily during exacerbations, with close monitoring of heart rate and blood pressure to avoid bradycardia or hypotension.
From a comparative standpoint, patients with stable septal hypertrophy often achieve better long-term outcomes with consistent medication adherence and lifestyle modifications. In contrast, those with waxing and waning patterns face higher risks of arrhythmias, heart failure, or sudden cardiac death due to the unpredictable nature of their condition. A study in the *Journal of the American College of Cardiology* found that patients with fluctuating septal thickness had a 2.5-fold increased risk of adverse events compared to those with stable measurements. This data reinforces the need for proactive management, including implantable cardioverter-defibrillator (ICD) consideration in high-risk cases.
Persuasively, clinicians must embrace a patient-centered approach that accounts for individual variability. For younger patients (under 40), lifestyle interventions—such as limiting strenuous exercise and managing stress—can mitigate waxing phases. In older adults (over 60), comorbidities like hypertension or diabetes may exacerbate fluctuations, requiring tighter control of these conditions. Practical tips include maintaining a symptom diary to track patterns, avoiding triggers like dehydration or alcohol, and ensuring regular follow-ups with a cardiologist.
In conclusion, the waxing and waning of septal hypertrophy demands a nuanced, data-driven strategy. By integrating frequent monitoring, flexible pharmacotherapy, and personalized lifestyle adjustments, clinicians can optimize long-term outcomes and reduce the risk of complications. This adaptive approach transforms the challenge of variability into an opportunity for precision care.
DIY Bikini Wax: Can You Safely Use Strips at Home?
You may want to see also
Frequently asked questions
Yes, septal hypertrophy can exhibit variability, with periods of worsening (waxing) and improvement (waning) depending on factors like underlying cause, treatment, and individual response.
Factors such as hypertension, valve dysfunction, volume overload, or changes in afterload can cause septal hypertrophy to fluctuate in severity.
Yes, in HCM, septal hypertrophy can vary due to disease progression, lifestyle changes, or response to medications like beta-blockers or disopyramide.
While it may improve significantly, complete resolution is rare unless the underlying cause is fully addressed, such as in cases of reversible hypertrophy due to hypertension.
It is typically monitored through regular echocardiograms, cardiac MRI, or other imaging studies to assess changes in septal thickness and cardiac function over time.